

Background/Case Studies: Bombay is a rare blood group characterized by the absence of H substance at
the surface of RBCs leading to naturally occurring anti-H antibodies. Anti-H presents the risk of severe
hemolytic transfusion reactions in these patients. The case presented is of a 32-year-old female of Middle
Eastern origin, who presented with a traumatic vertebral fracture with spinal cord compression and required
urgent neurosurgery. Her presenting hemoglobin was 84 g/L. She had no previous group and screen on
record, had never been transfused and had a history of a remote miscarriage.
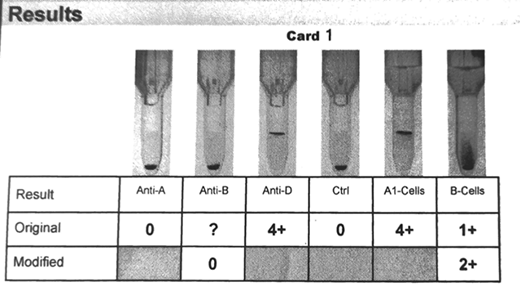
Study Design/Methods: Forward blood group with an automated gel-method instrument revealed the
following reactions: negative with anti-A, unable to interpret (?) with anti-B, 4+ with anti-D. Reverse
grouping revealed the following reactions: 4+ with A1-cells and an unexpected 1+ with B-cells. The antibody
screen and 11 cell panel in gel (Micro Typing Systems) 2+; the panel, with enhancement reacted 3+ in
Ficin. The auto control was negative. A second panel and pre-warm panel produced the same findings. An
antibody reacting at 37C against a high-frequency antigen was suspected. Patient specimen was sent for
investigation to the reference lab (RL), which performed blood group by manual tube test, antibody
identification with panels by manual tube PEG-IAT method; RL also sent a sample for ABH sequencing
(Sanger).
Results/Findings: A thawed frozen plasma sample from a previous Bombay patient 12 years prior showed
no reactivity against the patient's RBCs; positive control included. A frozen Bombay RBC unit was ordered
urgently from the blood supplier and was crossmatch compatible. The patient underwent surgery and was
transfused with a single unit of RBC for peri-operative bleeding. She was treated with erythropoietin and IV
iron post-operatively and did not require any further transfusions. The investigation at the RL showed mixed
field reaction on forward blood typing with anti-B and anti-A,B and negative reaction with anti-A commercial
reagents. The RL reverse grouping showed 4+ with all O H+ and A1 red cells, but 2+ with B cells. The autocontrol
and group O H- cells did not react, confirming anti-H and suggesting Para-Bombay group. ABH
sequencing revealed a normal B allele (ABO*B.01) while genotyping of FUT1 revealed a null allele
(FUT1*01N.12) and weak H allele (FUT1*01W.23). FUT2 genotyping (FUT2*01N.02) predicted a nonsecretor
(sese) phenotype.
Conclusions: This patient with non-secretor status, variant H production, clinically significant anti-H, greatly
reduced B antigen expression, should be treated as a Bombay (Oh) for transfusion purposes. She was
counselled and provided with an antibody card and a letter. This case illustrates the importance of timely
communication with the clinical team about the risks and benefits of transfusion pending antibody
identification, as it could have proved fatal in this case.
Pavenski:Bioverativ:Research Funding;Shire/Takeda:Honoraria;Octapharma:Research Funding;Alexion:Honoraria, Research Funding;Sanofi:Research Funding;Ablynx/Sanofi:Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal